A Rare Case of Metastatic Gall Bladder Polyp Secondary to Renal Cell Carcinoma
Abstract
Metastatic origin of Gall bladder polyp is usually associated with either gastric carcinoma or melanoma. Whereas, its association with Renal cell carcinoma is a rare occurrence. Its prevalence in autopsies is reported to be around 0.6%. Here, we present a case of 73-year-old gentleman, diagnosed with renal cell carcinoma 2 years back and underwent radical nephrectomy. During his routine follow-up, ultrasound revealed a gall bladder polyp which was about 28 mm in size. He underwent open cholecystectomy and histopathological analysis revealed it as a metastatic deposit. Hence, suggestive of metachronous gall bladder polyp in renal cell carcinoma.
Keywords
RCC: Renal Cell Carcinoma, Metachronous Disease, Fundic Lesion.
Introduction
Renal cell carcinoma (RCC) contributes around 80 percent of all kidney cancer cases. It is most often diagnosed during routine screening scans.[1] RCC has high grade metastatic potential and can be associated with synchronous or metachronous metastatic disease. The lag period between the occurrence of primary malignancy and metastasis can be as long as 10 years.[2]
Metastatic deposits in RCC are commonly seen at sites for RCC include lung, bone, liver and brain.
Gall bladder polyps are reported upto 6.9% in general population, whereas they are present in 0.6% in patients with Renal cell carcinoma. Usually GB polyps are incidentally detected on routine scans. In few cases they can present with vague and nonspecific symptoms. Various studies have shown malignant transformation of benign polyps. The risk is higher with age > 50 years and polyp size more than 1.5 cm. Thus, such polyps should be excised with cholecystectomy.
Here we present, a 73 year old male who was having Renal cell carcinoma since 2 years. He underwent nephrectomy at the time of diagnosis and was under regular follow up. During routine screening sonography, he was diagnosed with a polypoidal lesion in fundic region of gall bladder.
Case History
A 73 year old gentleman presented with a background history of radical nephrectomy and chemotherapy which were performed for renal cell carcinoma 2 years back. Patient was under regular follow up and had good performance status. Notably at the initial time of diagnosis there was no evidence of systemic or local metastasis.
During his routine follow up sonography, gall bladder is partially distended and shows a well-defined, non-mobile, predominantly hyperechoic lesion of size (2.8 x 0.8 cm) with evidence of vascular pedicle was seen in the fundus region of gall bladder. Simultaneously, there was no parenchymal lesion of liver. No abnormal peri-portal or para-aortic lymphadenopathy.

Contrast enhanced CT was further advised, which revealed a small isolated soft tissue density lesion (size 2.8 x 0.8 cm) showing homogenous bright enhancement on arterial phase imaging within the fundus of gall bladder. The soft tissue lesion was restricted to the gall bladder lumen and did not show any signs of invasion beyond the margins of gall bladder with surrounding peri-hepatic planes appearing unremarkable. There was no other abnormal enhancement involving the wall or any enhancing intra-luminal lesion seen involving rest of the gall bladder. No abnormal pericholecystic, coeliac, periportal or para-aortic lymphadenopathy seen. No definite metastatic deposit was seen in liver, both adrenals and in both kidneys.

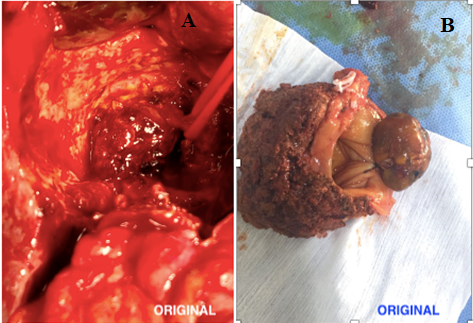
The patient was taken for cholecystectomy in view of large enhancing polypoidal lesion seen on CT scan. Per-operatively, gall bladder was removed and polyp was taken for frozen analysis. Histopathological examination revealed clear cells of renal carcinoma with delicate vascular stroma within the gall bladder polyp. The open cholecystectomy was later combined with extended segmental hepatectomy. The gall bladder polyp thus in given clinical background turned out to be a RCC metastasic deposit.
Discussion
Renal Cell Carcinoma (RCC) is a rare tumour accounting for less than 5% of all adult malignancies. It is normally discovered on routine screening. As RCC has high metastatic potential, it can normally present with a metastatic deposit at the time of initial diagnosis.
The survival rate of metastatic RCC is poor, with 1-year survival of less than 50%, 5 year survival of 5-30%, and 10 year survival of 0-5%.[3]
RCC is known to metastasize commonly to the lung, bone, brain, liver, or adrenal glands with metastasis to the gall bladder being extremely rare.
Very few case reports have been documented suggesting this rare localization.
In a study by Bennington et al. the incidence of gallbladder metastasis of RCC was reported to be 0.57% (3 out of 523 autopsies).[4] In another study Weiss et al. report 0.58% (4 out of 687 autopsies).[1]
Gallbladder has been known as a site for metastatic deposit for melanoma most commonly followed by lung, oesophagus, pancreas and colon carcinoma.[5] Hematogenous spread of metastasis from extraperitoneal organs like lung, breast, kidney and skin have been described.
Presence of Gall bladder polyp in sonograms in renal cell carcinoma can be due to both benign and neoplastic causes. Benign causes include cholesterol polyps, adenomyomatosis and inflammatory polyps while neoplastic causes include adenomas, primary gall bladder adenocarcinoma and metastatic deposit.
If on sonography, a gall bladder polyp is of size < 1 cm and doesn’t show any vascularity or associated thickening of gall bladder wall then these polyps are considered to be benign in etiology. Such polyps are followed up periodically and don’t require any immediate further investigation or intervention. But if the polyp is larger than 1 cm and shows prominent vessels within or shows infiltration of surrounding perihepatic planes, the polyp is considered to show alarming signs. These alarming signs raise a need for further investigation and intervention.[6,7,8]
In such cases, differentials to be considered should include cause like inflammatory polyp, adenoma, primary gall bladder adenocarcinoma or even metastatic deposits.
As in our patient, with an underlying history of RCC, finding of large gall bladder polyp with vascularity on routine scanning, raised the possibility of a potential neoplastic etiology. Radiological studies including ultrasonography and CECT described for metastatic renal cell carcinoma to the gallbladder are still unspecific as similar findings can be seen even in adenoma, primary gall bladder adenocarcinoma or even metastatic deposit from any other primary source. However, the finding of a large gall bladder polyp which shows accentuated arterial phase enhancement is useful in distinguishing metastatic GB tumor of RCC from primary GB tumor which is described to show heterogenous enhancement on contrast studies, similar is the case for metastatic deposits from any other primary.
Conclusion
Gall bladder polyps are secondary to various causes, however in background of a malignancy one should also consider metastatic polypoidal deposits.