Morphological and Morphometric Study of Pterion in Adult Dry Human Skulls
 1
,
Anjali
Jain
2
1
,
Anjali
Jain
2
Abstract
Introduction: Pterion is significant bony landmark because it commonly lies near the anterior branch of middle meningeal artery as well as Broca’s Area. The aim is to study the types of pterion and measure the distance from various bony landmarks on skull to the midpoint of pterion. Subjects and Methods: This study was performed on 70 adult dry human skulls of unknown age and sex. Types and location of pterion was observed bilaterally. Measurements were taken in millimeter using digital Vernier caliper from midpoint of pterion to i) fronto-zygomatic suture ii) middle of zygomatic arch iii) tip of mastoid process iv) glabella v) antero-superior margin of external acoustic meatus vi) Asterion. Results: We observed five types of pterion: spheno-parietal, fronto-temporal, stellate, epipteric and atypical. Among the skulls studied the most common type was sphenoparietal bilaterally. The mean of distances from midpoint of pterion to fronto-zygomatic suture was, 31.68±5.58 mm and 31.18±5.82 mm; to the middle of zygomatic arch was 38.87±3.63 mm and 37.84±3.99 mm; to asterion was 83.55±7.22 mm and 85.53±6.88 mm; to external acoustic meatus it was 51.70±3.20 mm and 51.37±3.39mm; to glabella it was 77.24±6.93 mm and 76.44±6.83 mm; to tip of mastoid process it was 80.77±6.10mm on the right side and 79.59±5.70 mm on the left side. Conclusion: Pterion is the most commonly used surface landmark. Findings of present study regarding classification of pterion will be helpful for neurosurgeons, radiologists, anthropologists and forensic pathologists.
Keywords
Middle Meningeal Artery, Asterion, Glabella
Introduction
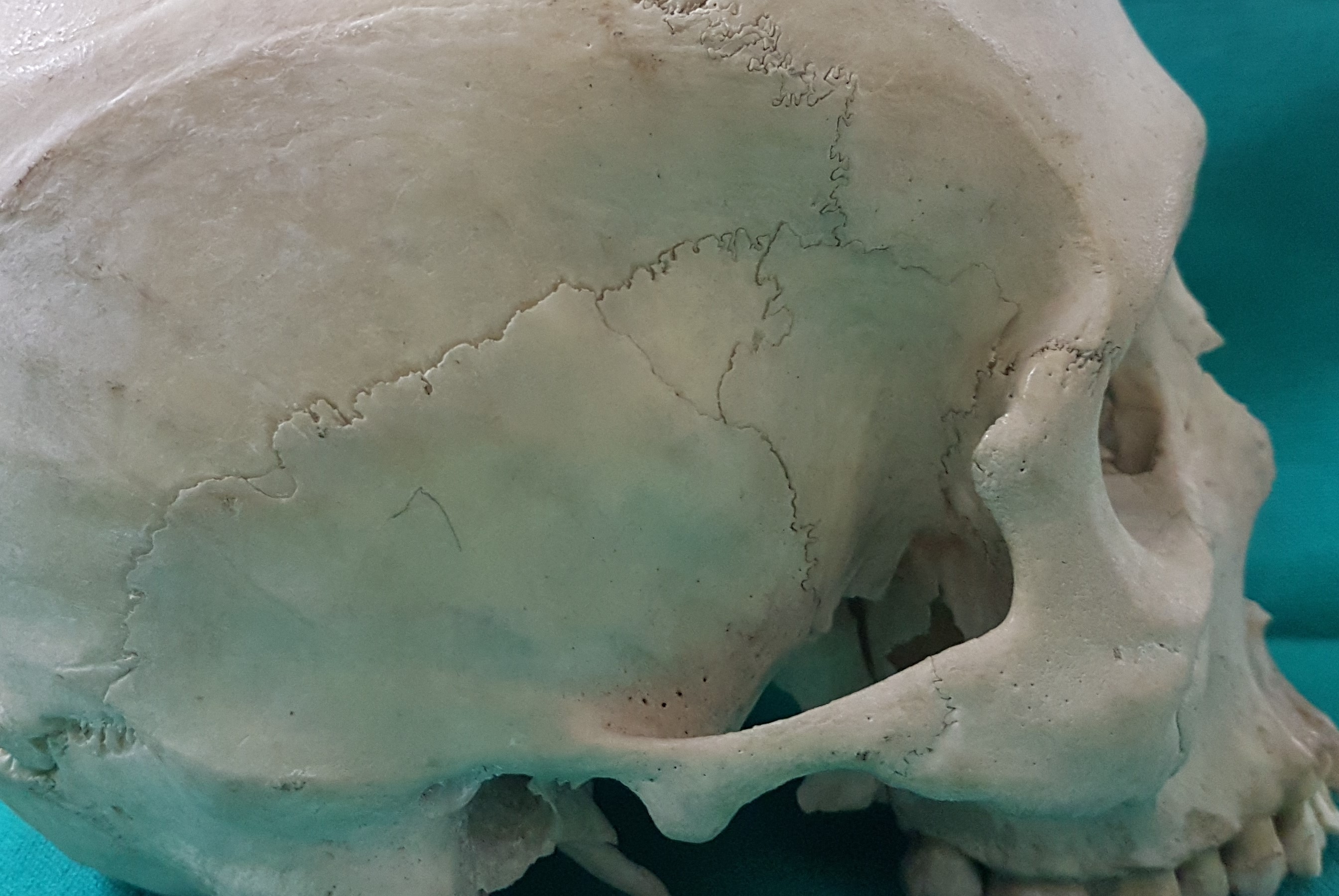
Four bones meet at sutural junction in floor of temporal fossa to form pterion i.e. frontal bone and parietal bone superiorly and greater wing of sphenoid bone and squamous temporal bone inferiorly. [1] Usually the group of sutures is H -shaped but variations occur and epipteric bone may be present. The centre of pterion lies approximately 4 cm above the zygomatic arch and 3cm behind the zygomatic process of the frontal bone. In this region the frontal branch of the middle meningeal artery lies in a groove on the inside of this bone and it is liable to be torn in fractures. [2] This is a major landmark in anthropometry because it overlies the middle meningeal artery (anterior branch) and Sylvian fissure of the cerebral hemisphere. [1]
It is essential to know the surface anatomy of pterion for correct positioning of burr-hole in pterional craniotomy done for removal of pituitary tumours. In archaeological studies and forensic specimens, the pterion serves as as an important guide for age estimation in suture closure methodology of cranium. [3] If wormian bones are present in the pterion region it may give a false impression of fracture and also sometimes real fracture may be interpreted as epipteric bone. Hence this must be known to radiologists. Knowledge about shape and location of pterion is of utmost important for neurosurgeons, anthropologists and forensic pathologists.
Subjects and Methods
Seventy dry skulls of adult humans irrespective of their age and sex were studied.
Inclusion criteria:
The present study included whole skulls and those in which vault of skull were cut but pterion and fronto-zygomatic suture were intact.
Exclusion criteria:
Skulls in which the shape of pterion was unclear due to damage or abnormal synostosis were excluded.
The shape of pterion was observed bilaterally and classified according to Murphy’s classification. [4] In order to measure distances from pterion to various bony landmarks, first centre of pterion was determined by using perpendicular bisectors theorem with the help of compass and lead pencil.
In sphenoparietal type of pterion, the suture between sphenoid and parietal bone was used as segment to find out the centre of pterion. One end of this suture was taken as centre, compass was placed here and arcs having more than half the length of the suture were drawn above and below. Then another end of the suture was taken as centre and arcs were drawn above and below. The point where both arcs intersected was joined by a thread. The line obtained was again intersected using perpendicular bisectors, the point where both these lines intersected were taken as centre of pterion.
In frontotemporal type of pterion, the suture between the frontal and temporal bone was used as segment. This segment was intersected using perpendicular bisectors theorem. In epipteric type of pterion, the point where frontosphenoidal and parietotemporal sutures meets the wormian bone was taken as centre and arcs were drawn taking radius more than half of length of wormian bone above and below.
In stellate type of pterion the point where all four bones meet was considered as midpoint of pterion.
Distances were measured in millimeter using digital Vernier caliper from midpoint of pterion to
i) Frontozygomatic suture
ii) Middle of zygomatic arch
iii) Tip of mastoid process
iv) Glabella
v) Antero-superior margin of external acoustic meatus
vi) Asterion.
The student’s t-test was applied to compare right and left side of the skull. The p-value > 0.05, this was considered not significant. The mean ± SD were calculated for various distances measured. Percentage of various types of pterion was calculated [Table 1]. Data was scrutinized using SPSS version 16.0.
|
Types of Pterion |
Right Side (n=70) in % |
Left Side(n=70) in % |
Both Sides (n=140) in % |
|
Sphenoparietal |
64.28% |
60% |
62.85% |
|
Atypical |
22.85% |
22.85% |
22.85% |
|
Epipteric |
11.42% |
14.28% |
12.85% |
|
Stellate |
1.42% |
1.42% |
1.42% |
|
Frontotemporal |
0% |
0% |
0% |
Results
The present study showed that Sphenoparietal type was the commonest. Second common type was atypical followed by epipteric and stellate. Frontotemporal type of pterion was absent. [Figure 1-5]




The distance from the midpoint of pterion to various bony landmarks on skull was measured to find out the exact location of pterion on the skull. The mean distances were tabulated in [Table 2].
|
Distances from midpoint of pterion to |
Right Side (Mean±S.D) in mm |
Left Side (Mean±S.D) in mm |
|
Posterior aspect of frontozygomatic suture |
31.68±5.58 |
31.18±5.82 |
|
Midpoint of zygomatic arch |
38.86±3.63 |
37.84±3.99 |
|
Asterion |
83.55± 7.22 |
85.53±6.88 |
|
Anterosuperior margin of external acoustic meatus |
51.70±3.20 |
51.37±3.39 |
|
Glabella |
77.24±6.93 |
76.44±6.83 |
|
Tip of mastoid process |
80.77±6.10 |
79.59±5.70 |
Discussion
Comprehension of the shape, location and relation of pterion to various bony landmark of skull is significant for neurosugeons while performing minimally invasive surgeries. The most common transcranial approach for removal of pituitary tumors is pterional or frontosphenotemporal craniotomy. It was made popular by Yasargil as the most widely used transcranial approach in neurosurgery for intracranial aneurysms nowadays. It provides direct accessibility to sella turcica and permits extraction of large pituitary tumors with minimal brain retraction. It is also the approach of choice for tumors such as a prefixed chiasma as it can be resected safely below the optic chiasma. [5] Therefore, the accurate location of pterion is mandatory. We took in consideration the Murphy’s classification of the pterion. Murphy et al reported that variations in shape of pterion are most likely due to environmental and genetic factors. [4]
The most common type of pterion in our study was sphenoparietal type which was similar to all other past studies. During evolution of primates, the anterosuperior part of the squamous temporal bone of lower primates became detached and in humans it fused with the posterosuperior angle of the greater wing of the sphenoid bone, thereby changing the shape of pterion from the frontotemporal type of lower primates to the sphenoparietal type of humans. Second common type of pterion found was atypical type which was not seen in any other past studies except by Satpute et al, [6] who observed 1.76% atypical type in his study. Third common pterion type observed in the present study was epipteric type which was much less in comparison to other studies done on north Indian population, whereas it was similar to studies done on west indian population by Zalawadia et al. [7] Next common type of pterion was stellate type which was similar in all indian studies, but in a study done by Lee et al, [8] on Korean population it was absent. The frontotemporal type was absent in the present study, which was same as that of Lee et al. [8] [Table 3]
|
Authors |
Types |
||||
|
Spheno-parietal |
Atypical |
Epipteric |
Stellate |
Fronto-temporal |
|
|
Murphy et al (1956), [4] |
73% |
- |
1% |
18.5% |
7.50% |
|
Aggarwal et al (1980), [9] |
93.48% |
- |
23.34% |
2.17% |
4.35% |
|
Lee et al (2001), [8] |
76.5% |
- |
23.50% |
0% |
0% |
|
Saxena et al (2003), [10] |
84.72% |
- |
0% |
5.17% |
10.01% |
|
Mwachaka et al (2009), [11] |
66% |
- |
12% |
7% |
15% |
|
Satpute et al (2013), [6] |
82.94% |
1.76% |
7.05% |
5.29% |
2.94% |
|
Seema et al (2014), [12] |
89% |
- |
12% |
4% |
7% |
|
Gindha et al (2016), [13] |
72.31% |
- |
23.08% |
0% |
4.61% |
|
Present study (2018) |
62.85% |
22.85% |
2.85% |
1.42% |
0% |
Similarities were observed in the location of pterion as the mean distance from the midpoint of pterion to several bony landmarks and was found similar to the studies done in other indian population as well as that done in a study done by Aymen et al in Saudi Arabia. [14]
|
Author |
Distance(Mean±S.D) in mm |
|||||||
|
P-FZ |
P-ZA |
P-EAM |
P-Ms |
|||||
|
Right |
Left |
Right |
Left |
Right |
Left |
Right |
Left |
|
|
Ilknur A et al (2009), [3] |
35±5.0 |
35±5.0 |
39±9.3 |
39±5.0 |
58±4.0 |
51±4.0 |
77±5.0 |
78±5.0 |
|
Aksu F et al (2014), [15] |
31.80±4.5 |
31.44±4.7 |
40.02±4.06 |
39.88±4.0 |
53.29±4.5 |
56.22±4.6 |
82.48±5.45 |
81.81±5.5 |
|
Seema et al (2014), [12] |
31.0±4.4 |
34.0±4.0 |
41.0±4.5 |
44.0±3.2 |
-- |
-- |
-- |
-- |
|
Prasad H et al (2015), [16] |
32±3.9 |
31.1±4.0 |
37.1±3.9 |
36.8±3.5 |
51.9±5.9 |
51.2±3.2 |
80.2±5.8 |
81.3±4.5 |
|
Aymen A et al (2016), [14] |
32.3±3.9 |
31.2±5.0 |
36.3±3.5 |
37.3±3.1 |
51.8±5.6 |
51.3±3.3 |
81.3±5.3 |
81.2±4.4 |
|
Gindha et al (2016), [13] |
38.71±3.1 |
36.29±3.7 |
39.00 ±2.5 |
37.00±3.3 |
-- |
-- |
-- |
-- |
|
Kulkarni P et al (2017), [17] |
29.81±4.4 |
29.81±4.0 |
37.16±3.77 |
37.56±3.7 |
53.40±7.2 |
53.57±6.7 |
80.35±3.4 |
80.96±3.7 |
|
Present study |
31.68±5.5 |
31.18±5.8 |
38.86±3.63 |
37.84±3.9 |
51.70±3.2 |
51.37±3.4 |
80.77±6.10 |
79.59±5.7 |
There were regional differences in these distances when compared between Indian and Turkish population. In a study done in solan by Gindha et al, [13] the distance from centre of pterion to frontozygomatic suture was very high as compared to the present study this can be explained based on the fact that the development of skull depend on genetics of particular race. [Table 4]
Conclusion
We concluded that sphenoparietal type is the most commonly found type and frontotemporal type was usually either absent or less common in human population in all ethnic groups, this fact can be used by anthropologists to study the bony remains. Mean linear distances of pterion from various cranial bony landmarks derived in this study will be of great help in determining the exact point for burr-hole positioning while performing craniotomy. Also, more no. of epipteric bone in pterion region is an indication of rapidly growing cranium as seen in hydrocephalus.
Acknowledgment
All the authors acknowledge the help that we received from authors of various articles which are cited in the reference of this manuscript. We are very grateful to all the technical help involved in this study.